Artigo especial em inglês para o WHR
Dr David Redwine explica porquê a endometriose não é menstruação retrógrada
Dr David Redwine é médico e pesquisador da endometriose - Bend, Oregon - Estados Unidos - Agosto de 2023 - All rights reserved
Original paper vol (1) pg1
Mulleriosis: The best-fit theory of origin of endometriosis
The origin of endometriosis is important because rational treatment would emerge if the cause of the disease were known. The medical literature continues to be filled with descriptions of endometriosis as a “confusing, mysterious, enigmatic disease” affecting around 10% of females worldwide. Such uncertainty after so much study for over a century is a clear indication that basic assumptions about the disease must be wrong.
And what could be more fundamental about a disease than its origin? The confusion surrounding endometriosis must include some error in our understanding of its origin. Since Sampson’s theory of reflux menstruation is the most commonly cited cause of endometriosis, the trail of confusion points directly at this theory, incriminating it as a main cause of confusion.
The fatal flaws of reflux menstruation as the origin of endometriosis
Sampson’s theory of reflux menstruation says that during the menstrual flow some menstrual fluid escapes out of the fimbriated ends of the tube, dripping blood, endometrial cells, and endometrial tissue fragments into the peritoneal cavity where the refluxed tissue attaches to peritoneal or other surfaces, proliferates upon and invades those surfaces to become the disease called endometriosis. And during any year, this process must be occurring literally by the billions when you consider that 10% of menstrual-aged females around the world have endometriosis.
The components of menstrual fluid include erythrocytes, stromal cells, and glandular cells is shown in Figure 1.

Erythrocytes have a dimension of 8 microns (µ). There is little variation in normal erythrocytes, so in viewing photomicrographs, erythrocytes serve as a convenient measuring stick for other cells. A capillary is about 10 µ in diameter.
Endometrial stromal cells have a dimension of about 20 µ, and taller glandular cells have a dimension of about 75 µ. Of course there is variation in size of endometrial cells, so these are just typical dimensions for the sake of this discussion. Since cells may shed singly or in clumps of tissue, we could take the dimensions of stromal and glandular cells and estimate a theoretical size range of refluxed tissue clumps: stromal tissue clumps might have several cells easily adding up to 100 µ in dimension, while larger glandular cells clumped together might be 200 µ or greater in size, as might be combinations of the two cell types. The largest theoretical size of refluxed endometrial tissue fragments would be limited by the smallest diameter of the fallopian tube, which is less than 1 mm in the intramural portion of the uterus.
This means that reflux menstruation would theoretically result in endometrial cells and tissue fragments ranging in size from about 20 µ (a single stromal cell) to about 900 µ (smallest inner diameter of fallopian tube) escaping to implant on pelvic surfaces. A human hair is 100 µ in diameter and can be easily seen at arm’s length and a human hair is smaller than a typical lesion of endometriosis as shown in Fig 2.

Just because something is viewed through a microscope does not make it invisible to the unaided eye. This means that most refluxed tissue fragments would be visible to the naked eye.
The only acceptable scientific proof of Sampson’s theory of reflux menstruation would be to see a large number of photomicrographs showing in detail the sequential steps of attachment, proliferation, and invasion. Given the prevalence of endometriosis and the great interest in its study over the last 150 years, our textbooks should be filled with photomicrographs showing these missing steps. And this is the fatal flaw of Sampson’s theory: the proof would be very easy to obtain, so the absence of any evidence of the missing steps can be taken as proof that the origin of endometriosis is not reflux menstruation because the evidence would be impossible to miss if it occurred. The only ‘evidence’ for the theory of reflux menstruation is in the form of cartoons, Figure 3.

The lack of photomicrographic proof of these three steps cannot be explained rationally. Virologists can photograph the spikes on covid and astronomers can photograph huge supernova remnants (Figure 4).

Yet within the visible spectrum relating to reflux menstruation, there is supposedly a size range between 20 and several hundred microns which cannot be photographed? This is an unacceptable insult to science and to patients whose medical care is influenced by cartoon science. Reflux menstruation can be rejected as the origin of any form of endometriosis.
Since reflux menstruation can’t be scientifically accepted as the origin of endometriosis, various arms of the theory are also invalid:
Hematogenous dissemination: At 20 µ in diameter, an endometrial stromal cell is the smallest endometrial cell which would enter the venous circulation. This cell is at least twice as large as the diameter of a capillary. Since 100% of venous blood eventually goes through the lungs, 100% of endometrial cells entering any pelvic vein would be filtered out by the 10 µ filter of the pulmonary capillary bed, in which case there should be a high prevalence of parenchymal pulmonary endometriosis, which there is not. And on the arterial side of the circulation, any endometrial cells or tissue fragments which magically made it past the lungs – whether through a patent ductus arteriosis or atrioventricular septal defect - should accumulate preferentially in organs with a greater percent of the cardiac output, such as the brain and kidneys. The pelvis gets less than 10% of cardiac output, yet it is overwhelmingly the favored location of endometriosis. Hematogenous spread can be rejected on the basis of simple hydraulics.
Deficient immune system: a competent immune system theoretically fights off refluxed endometrial cells, protecting patients from endometriosis. But where are the photomicrographs of this immunologic warfare occurring in the pelvis of patients who don’t develop endometriosis? We should see refluxed cells undergoing phagocytosis by leukocytes and lytic destruction in the 90% of patients with a normal pelvis who don’t develop endometriosis. So this must be occurring very frequently so evidence should be easy to come by. But just as we don’t see photomicrographs of the missing steps of reflux menstruation, we don’t see the photomicrographs of this presumed immunological warfare either. Patients with endometriosis by and large have a normal, competent immune system and most don’t have autoimmune diseases or cancer. Since there is no evidence of a competent immune system army destroying refluxed cells in the pelvis of patients without endometriosis, it would be illogical to go out on a tree limb and propose a corresponding situation where a deficient immune system is blamed for contributing to the development of endometriosis in patients with the disease. There simply is no evidence. The deficient immune system arm of reflux menstruation can be rejected.
Peritoneal circulation: evidence for a peritoneal circulation directing the deposition of refluxed cells and tissue fragments was borrowed from a radiological tilt-table study by Meyers of males with acute intraperitoneal pathologies including abscess, peritonitis, cancer, and adhesions. In Meyers’ study, radio-opaque dye was injected into the peritoneal cavity and the path of the dye was followed by fluoroscopy. The radiological study resulted in a schematic diagram of the abdominal cavity with arrows going in many directions depending on the tilt of the table, Figure 3a. Modern authors supporting reflux menstruation showed that if they took Meyers’ diagram and gratuitously erased some arrows and added others, they could manufacture evidence of a clockwise circulation (as one looks at the patient) which they felt would explain a slightly higher prevalence of endometriosis of the left uterosacral ligament and left ovary and a higher prevalence of right diaphragmatic involvement (Figure 3b).
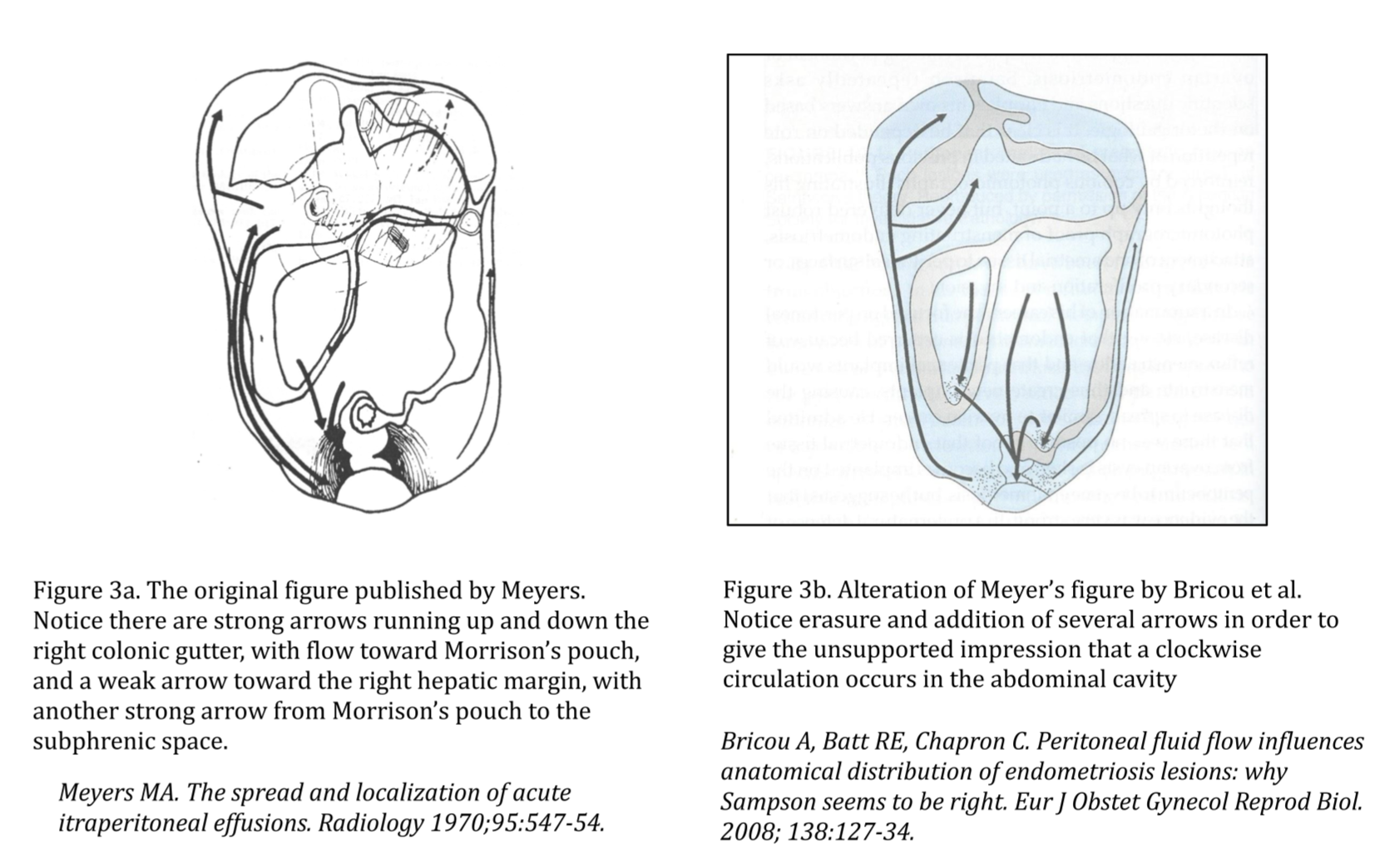
Since the only evidence in support of a peritoneal circulation arm of reflux menstruation is fabricated, this arm of reflux menstruation can be rejected.
Autotransplantation of endometrium during c-section or other surgeries: Scar endometriosis most commonly manifests as a single nodule centered on the level of the rectus fascia, with some penetration of fat anteriorly and occasionally some penetration into the anterior retroperitoneum. Considering that the entire c-section wound is saturated with amniotic fluid, blood, and endometrial tissue, one would expect patients to have multiple areas of scar endometriosis, from skin down to the region of the bladder, from the left side of a transverse incision to the right side. An occasional single nodule of scar endometriosis is not supportive of widespread contamination of a surgical scar by disseminated decidual endometrium. Scar endometriosis has another possible origin, so contamination during c-section can be rejected.
And of course if one believes in reflux menstruation, one must also believe in at least one other theory of origin to explain endometriosis in males.
The question: Was Sampson wrong? The answer: Yes, obviously
If not reflux menstruation, then what?
A unified theory of origin must explain everything we know about endometriosis and lead to answering what we don’t know.
Here are some basic facts about endometriosis that are necessary in formulating a theory of origin:
We know that disease in young patients can be colorless and very subtle, but can change in color appearance with the passage of time: some (but not all) such early lesions may produce glandular secretions which leach through tissue and destabilize adjacent capillaries, causing local microbleeding and a red appearance.

Some more irritative lesions may stimulate angiogenesis while others may stimulate overlying fibrosis, thus resulting in a yellowish or whitish coloration. When dark hemorrhage is seen beneath a nodular fibrotic surface, this would represent a ‘black powderburn lesion’ phenotype, often associated with endometrioma cysts. This was the classic presentation of endometriosis which predominated in the literature before 1985.
Selection bias for advanced age was typical of publications of the early 20th century because the early subtle forms of the disease were virtually completely overlooked. So in addition to a faulty main theory of origin, endometriosis has been severely affected by selection bias which ignored younger patients with more subtle manifestations.
We know that older age groups don’t have more areas of pelvic involvement than younger age groups, suggesting that endometriosis is somewhat geographically static in the pelvis over time.
Endometriosis occurs in repetitive patterns. Experienced endometriosis surgeons may experience a sense of ennui after having performed their 3,000th case because they realize that they are seeing the same patterns of disease over and over again. The patterns are consistent. They are not random. Von Rokitansky noted these patterns and commented that deep endometriosis occurs in tissues with muscle fibers, such as bowel, bladder and uterosacral ligaments. He was noting in this way that endometriosis has static ‘favored’ locations which are not random.
The patterns of endometriosis extend outside the pelvis, e.g. 10:1 ratio of right diaphragmatic endometriosis to left as well as predictable patterns of bowel and bladder involvement.
Endometriosis occurs in the pelvis of elderly males receiving estrogen for palliation of advanced prostate cancer, including the bladder and prostate.
As shown by reoperations, endometriosis can be cured in over 50% of patients by aggressive excision. Most of the rest have less disease.

Recurrent disease following excision is uncommon but is typically superficial and minimal.

Endometriosis has been found in the pelvis of an infant female, in abortuses, in fetuses.

Several primate species splitting from the human clade 2 – 25 million years ago develop endometriosis:
- Baboons 2,000,000 years ago
- Macaques 7,000,000 years ago
- Cynomolgus monkeys 10,000,000 years ago
- Rhesus monkeys 25,000,000 years ago.
Endometriosis has protean possible manifestations in every possible realm – phenotype, malignant potential, hormone receptors, symptoms, invasive potential, etc, etc. A unifying theory must account for limitless possible combinations and permutations, so such a theory would necessarily be associated with the use of mathematics and supercomputers.
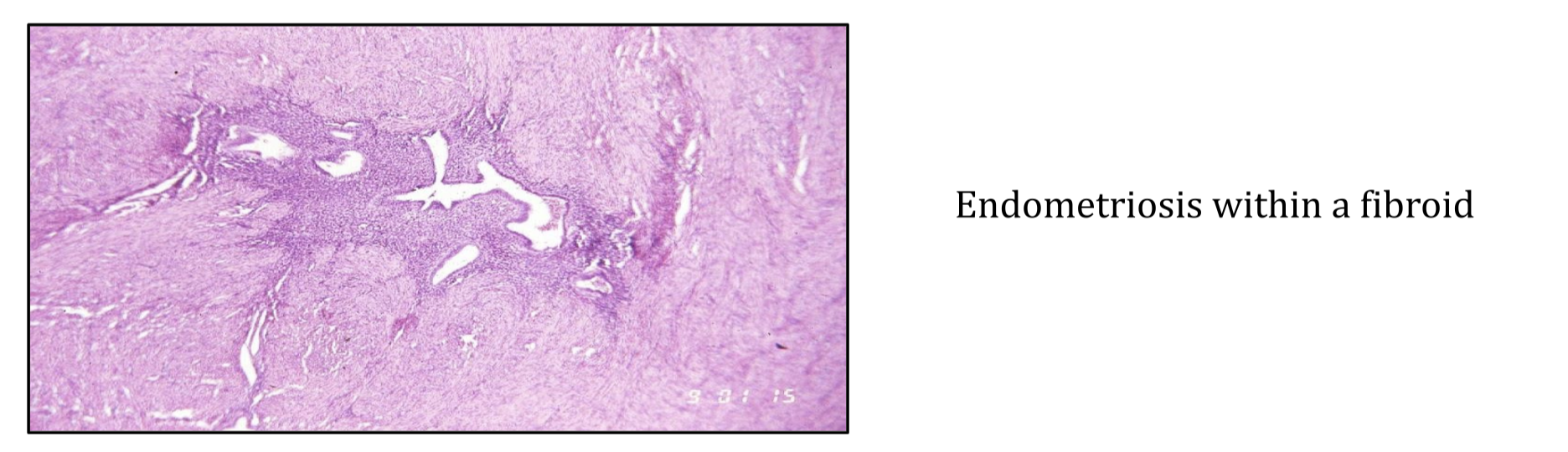
Endometriosis is correlated with adenomyosis clinically and histologically. Endometriosis can occur in the middle of a leiomyoma, so it is correlated with fibroids as well.
Endometriosis is associated with structural defects of the urogenital system, including uterine fusion defects, peritoneal pockets, cervical stenosis and renal agenesis. A unifying theory must explain these associations.

A unifying theory must also explain why Sampson’s theory is missing important photomicrographic evidence of attachment, proliferation and invasion.
A unifying theory of origin of endometriosis
Well by now you’ve guessed that the origin of endometriosis cannot be reflux menstruation so the origin must be a genetically-driven process that begins at the moment of conception, is expressed during embryogenesis and is eventually manifest with exposure to estrogen. It’s a pretty simple and straightforward conclusion when you look at real facts. But the situation is complicated by the fact that there are dozens or hundreds of genes that have been identified to have some association with endometriosis. These genes allow the limitless manifestations of disease but complicate its study, requiring math and supercomputers. Stay tuned to genetics because this will be where progress and insight will occur. Of interest, geneticists will depend on excised tissue, so excision will continue to lead the way.
Genetics combined with basic embryology =e ndometriosis and related diseases: Mulleriosis
When an egg and sperm unite, the process to form endometriosis is set in motion. It depends on genetics, chance, and perhaps the environment.
The embryo has 3 layers that look like ravioli on cross section – the top is ectoderm (which forms CNS and skin); the bottom layer is endoderm (which forms GI and GU mucosa) and mesoderm is in the middle and forms everything else in the body. This means that all endometriosis is from mesodermal origin. This explains why the GI and GU mucosa are not primarily involved by endometriosis. During gastrulation, epiblast cells travel through the primitive groove to become mesoderm sandwiched between the ectoderm on top and the endoderm on bottom.
Depending on the genetics of an individual patient, the differentiation and migration of tissue during embryogenesis will be affected, resulting in patterned tracts of deposition of two main types of cells: 1. islands of endometriosis. 2. surrounding stem cells with weak genetic tags for endometriosis. Because pelvic organogenesis proceeds down the posterior coelomic cavity in the embryo, these tracts are concentrated in the posterior pelvis, explaining the most frequent sites of occurrence. But lesser tracts can be located anywhere in the body, including the anterior abdominal wall where stem cells laid down during embryogenesis can be stimulated by the growth factors of surgical healing following c-section and so provoked to form a nodule of scar endometriosis.
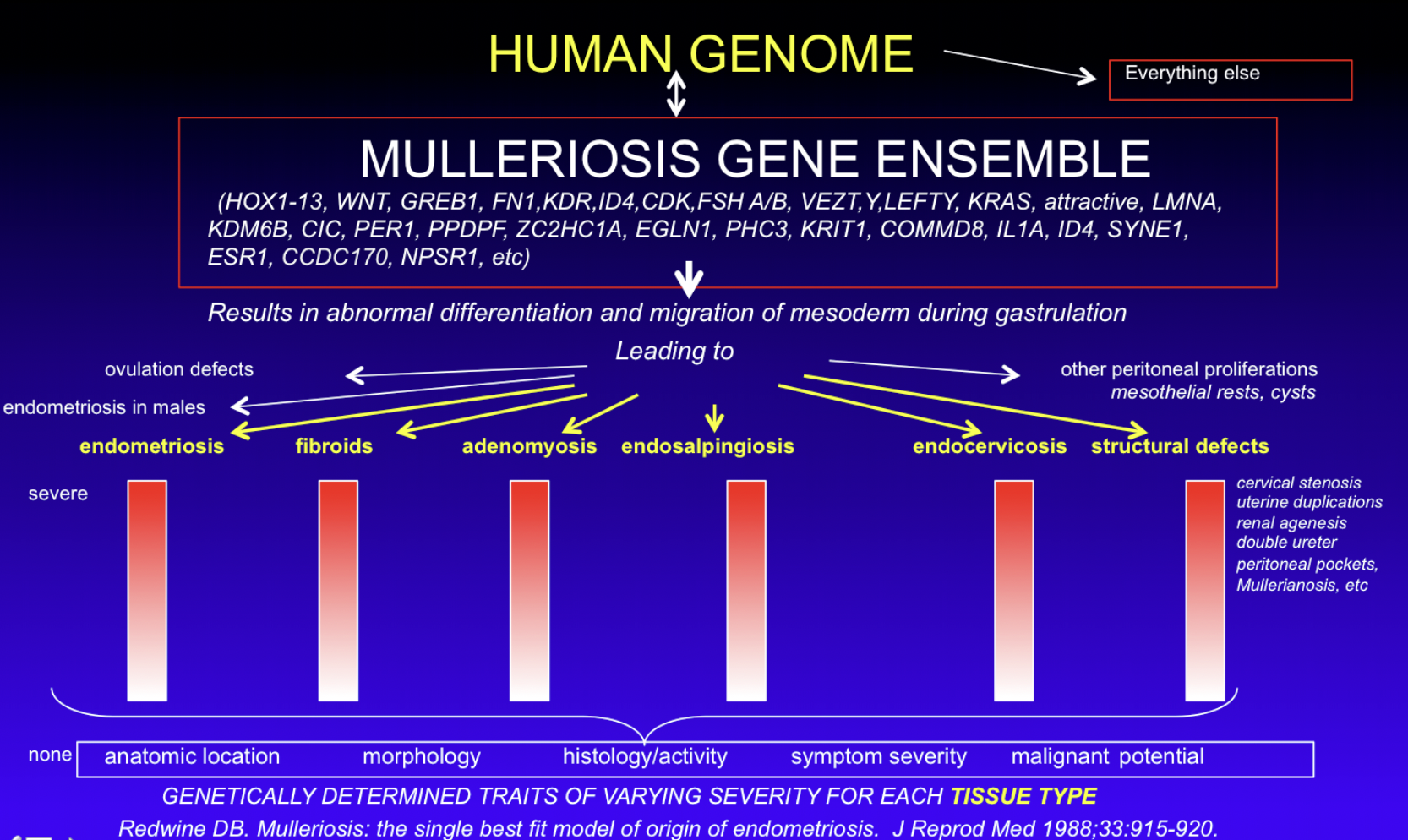
The problems of differentiation and migration are not limited to endometriosis and can include other gyn pathologies and the related structural problems. They are ontologically related because they are genetically related. These genetically-determined embryologically-patterned tracts will be wherever the genes drive them. HOX genes play a large role and the repetitive macro- and micro-patterns seen so frequently by endometriosis surgeons are likely governed by an array of lesser genes, all inter-related. Since endometriosis is related to other gyn diseases with overlapping symptoms, histology and genetics, it can be postulated that there is a Mulleriotic Gene Ensemble that is responsible for endometriosis and its related pathologies. I invented the term ‘Mulleriosis’ to invite scientists to look ‘higher up the genome’ at a broader spectrum of related diseases and structural defects instead of focusing on endometriosis alone.
Endometriosis can be stimulated by estrogen as puberty approaches. Pain is the most common and most specific symptom of the disease. Endometriosis is highly variable in all its aspects. There’s a gene for that. Actually hundreds of genes for that. The interaction of genes at conception and beyond is more than sufficient to result in any identifiable trait exhibited by endometriosis. Just because we don’t have all the genetic answers yet is not a reason to embrace reflux menstruation and cartoons. Symptomatic patients undergoing excision can be cured of endometriosis if all visible lesions and adjacent stem cells are removed. Of course, there is no way to know how far from a visible lesion stem cells might exist. This is why endometriosis surgeons perform wide local excision, to increase the chance of removing nearby stem cells with genetic tags to form superficial recurrent disease. If all visible lesions but not all adjacent stem cells are removed, then superficial local recurrence is possible. So Mulleriosis would explain the results seen after excision. A genetic/embryonic origin would explain the occurrence of endometriosis in abortuses, fetuses, and an infant female. A genetic origin also perfectly satisfies the impossible-to-photograph missing steps of Sampson’s theory because you can’t photograph genes with a typical light microscope. Sampson’s theory is a lame proxy for a genetic/embryonic origin. It was not great in its time, but it’s time is gone.
The Future
Mulleriotic Gene Ensemble screening test
Each newborn will have full genotyping performed, which will include investigation for a Mulleriotic Gene Ensemble (MGE). Endometriosis patients will have MGEs which are similar but which carry distinctive differences. A child’s MGE will be used to predict who will have disease of what type and in what location. Prophylactic excision of predicted tracts may prevent future disease. Future disease staging systems will include those based on genetics rather than scans or surgical findings. Genetics may eventually unlock a genetic treatment, but until then, excision will remain the best treatment for any patient of any age with any symptom due to endometriosis.
Should we say “I’m sorry”?
When you consider the number of patients with endometriosis and the number who have been poorly treated in some way based on Sampson’s theory, whether medically or surgically, you can begin to understand the tremendous insult this has been to patients and to science. This makes the theory of reflux menstruation as the origin of endometriosis the most dangerous theory in the history of medicine. And it continues. We have allowed cartoonists to guide us. Cartoons have become scientific evidence. This is worse than the Emperor’s New Clothes – the Emperor was only embarrassing himself by denying the obvious. We are damaging patients by denying the obvious: reflux menstruation is not the origin of any form of endometriosis. To any supporter of reflux, I say simply ‘Show me the pictures.’ So what do we say to several generations of hundreds of millions of patients who have been adversely affected in some way by cartoon science? “I’m sorry” seems like such an empty phrase, but it’s a start. Until the profession acknowledges the depth of harm to patients and science caused by adherence to reflux menstruation, a moral cloud will hang over the profession which cannot be lifted. The simplest way forward in the study of endometriosis is to completely reject reflux menstruation and anything based on it. This can be done for free and would have an immediate huge impact because all energy and thought can be toward a more likely direction. One of the tenets of Mulleriosis is the specific rejection of Sampson’s theory of reflux menstruation as the cause of any form of endometriosis. With Mulleriosis, we don’t need Sampson. But we do need more excised tissue for genomic studies and supercomputers to put it all together.

Ref.:
- Redwine Was Sampson wrong? Fertil Steril. 2002 Oct;78(4):686-93.
- Batt RE, Smith RA, Buck Louis GM, Martin DC, Chapron C, Koninckx PR, Yeh J. Müllerianosis. Histol Histopathol. 2007 Oct;22(10):1161-6.
- Redwine Endometriosis and autoantibodies. Fertil Steril. 1989 Jun;51(6):1068-9.
- Chiminacio I, Obrzut How to Remove Endometriosis? Removing All Peritoneum from the Pelvic Compartment: En Bloc Peritonectomy, a Demonstration of the Technique. Journal of Minimally Invasive Gynecology. Volume 29, Issue 11, Supplement, 2022, Page S57.
- Redwine DB. ‘Invisible’ microscopic endometriosis: a review. Gynecol Obstet Invest. 2003;55(2):63-7.
- Salmeri N, Gennarelli G, Vanni VS, Ferrari S, Ruffa A, Rovere-Querini P, Pagliardini L, Candiani M, Papaleo Concomitant Autoimmunity in Endometriosis Impairs Endometrium-Embryo Crosstalk at the Implantation Site: A Multicenter Case-Control Study. J Clin Med. 2023 May 19;12(10):3557.
- Casals G, Carrera M, Domínguez JA, Abrão MS, Carmona F. Impact of Surgery for Deep Infiltrative Endometriosis before In Vitro Fertilization: A Systematic Review and Meta-analysis. J Minim Invasive Gynecol. 2021 Jul;28(7):1303-1312.e5.
- Marquardt RM, Kim TH, Shin JH, Jeong JW. Progesterone and Estrogen Signaling in the Endometrium: What Goes Wrong in Endometriosis? Int J Mol Sci. 2019 Aug 5;20(15):3822.
- Batt RE, Yeh Müllerianosis: four developmental (embryonic) mullerian diseases. Reprod Sci. 2013 Sep;20(9):1030-7.
- Signorile PG, Baldi F, Bussani R, Viceconte R, Bulzomi P, D’Armiento M, D’Avino A, Baldi A. Embryologic origin of endometriosis: analysis of 101 human female fetuses. J Cell Physiol. 2012 Apr;227(4):1653-6.
- Chiminacio I, Obrzut C, H Sabadin Posterior Compartment Peritonectomy: Technique Demonstration Journal of Minimally Invasive Gynecology. Volume 29, Issue 11, Supplement, 2022, Page S59.
- Agarwal SK, Chapron C, Giudice LC, Laufer MR, Leyland N, Missmer SA, Singh SS, Taylor Clinical diagnosis of endometriosis: a call to action. Am J Obstet Gynecol. 2019 Apr;220(4):354.e1- 354.e12.
- Lorusso F, Scioscia M, Rubini D, Stabile Ianora AA, Scardigno D, Leuci C, De Ceglie M, Sardaro A, Lucarelli N, Scardapane A. Magnetic resonance imaging for deep infiltrating endometriosis: current concepts, imaging technique and key findings. Insights Imaging. 2021 Jul 22;12(1):105.
- Horne AW, Missmer Pathophysiology, diagnosis, and management of endometriosis. BMJ. 2022 Nov 14;379:e070750.
- Possover M, Andersson KE, Forman A. Neuropelveology: An Emerging Discipline for the Management of Chronic Pelvic Pain. Int Neurourol J. 2017 Dec;21(4):243-246.
All rights reserved - David Redwine - With authorization for WHR - Woman's Health Research - Endometriosis Brazil